La société française de capital-risque Karista a publié son étude annuelle sur les investisseurs européens dans les start-up de santé...-Start-up...
Via Doc-Ifsi-Narbonne
Get Started for FREE
Sign up with Facebook Sign up with X
I don't have a Facebook or a X account


 Your new post is loading...
Your new post is loading... Your new post is loading...
Your new post is loading...
La société française de capital-risque Karista a publié son étude annuelle sur les investisseurs européens dans les start-up de santé...-Start-up... Via Doc-Ifsi-Narbonne 
No comment yet.
Sign up to comment

Une vingtaine de cabinets de médecine générale aux Pays-Bas, ont installés sur leurs sites web une nouvelle interface clinique utilisant l'intelligence artificielle (IA) pour une réponse rapide à des patients en première ligne qui se posent des questions sur des symptômes de santé. Elle montrerait des avantages considérables,pour réduire les angoisses du patient et préparer un rendez-vous médical. Via Philippe Marchal

PARIS--(BUSINESS WIRE)--Tilak Healthcare, a leading company in digital health for the monitoring of chronic eye diseases, announces the appointment of three experts to support the leadership team, currently composed of Edouard Gasser (CEO & co-founder), Philip Bouchet (Chief Operating and Product Officer), and Dr. Bénigne Mathieu (Chief Business Officer). These appointments mark a crucial milestone in the evolution of Tilak Healthcare, currently in hypergrowth (+100% prescriptions in 2023), Via Emmanuel Capitaine
From
www

To make health systems more sustainable in the long-term, incentivize artificial intelligence (AI) and digital technologies that are grounded on careful testing and real-world validation. Via Emmanuel Capitaine
$post.getHtmlFragment()
Lire l'article complet sur : parisantecampus.fr
Lionel Reichardt / le Pharmageek's insight:
Ravi de travailler avec lui sur Axelife depuis deux ans..
TICpharma.com est un site d'informations sur la transformation digitale des industries de sant�.
From
www
See Chai Carol Chan, academic clinical fellow in general practice, Ana Luisa Neves, clinical senior lecturer in digital health, director of Global Digital Health Unit, Azeem Majeed, professor of primary care, & public health, Aldo Faisal, professor of artificial intelligence and neuroscience, Department of Computing and Department of BioengineeringImperial College LondonRapid advances in artificial intelligence (AI) are paving the way for innovations in how healthcare is delivered. AI technologies have shown remarkable potential in outperforming humans in diagnosing a range of clinical conditions including cancer, diabetes, cardiac arrhythmias, and Alzheimer’s Disease.1 To date, the UK Department of Health and Social Care has invested £123 million directly into 86 AI technologies and have allocated an additional £21m in October 2023 to 64 NHS hospital trusts in England, aiming to streamline diagnostic procedures, enhance predictive analytics, and ultimately improve healthcare delivery and patient outcomes.2 In addition, AI can help democratise access to world-leading expertise distilled into algorithms, and bring underserved, often rural communities, health and care support that would be difficult to realise otherwise.The promise of AI comes with significant considerations regarding equity, which we define as fair access to medical technologies and unbiased treatment outcomes for all population groups based on clinical need. These issues include data representation, algorithmic bias, accessibility of AI-driven technologies, and the implications of these technologies for patient outcomes across diverse population groups. In particular, the quality and inclusivity of data on which AI tools are trained on are often problematic, because clinical data used by businesses or researchers often cannot be vetted.The overall fragmentation of data availability thereby results in less representative data and a lack of universally agreed data collection standards.3 Additionally, we must acknowledge the complexities surrounding race and ethnicity in healthcare data. Under-representation of certain demographics in training datasets can lead to biases in AI models. Existing medical technologies and devices have highlighted that AI can be less accurate at diagnosing diseases in people from ethnic minority groups. The use of race or ethnicity as variables in clinical risk prediction models can perpetuate existing healthcare discrimination. For instance, the controversial race-based correction factor used in estimating glomerular filtration rate (eGFR) for assessing kidney function in chronic kidney disease patients can delay diagnosis and treatment for Black populations.4 Beyond ethnic biases, clinical conditions often present differently between genders. Women are more likely to be under-diagnosed in cardiovascular diseases and under-represented in cardiology research, so current evidence-based medicine can be misrepresentative. AI diagnostic tools therefore must be developed with gender-balanced data to avoid perpetuating existing gender health disparities.5 Tackling these biases in predictive models and health research is a priority, as AI has the potential to both replicate and resolve these long-standing inequities.Transitioning from principle to practice for AI to achieve equity is a complex task with no singular solution; it requires a multi-dimensional, systems approach, rooted in a strong ethical foundation. The ethical guidance developed by the World Health Organisation in 2021 emphasises the importance of inclusivity, transparency, and accountability in AI for healthcare.6 Drawing upon this guidance, it is crucial to scrutinise and modify AI tools at various stages, including problem selection, data collection, outcome definition, algorithm development, and post deployment.7 Each of these stages presents an opportunity to embed equity-centred considerations. For instance, during the problem selection stage, we can identify and prioritise health issues that disproportionately affect marginalised communities. Similarly, we need to ensure diversity in data collection, adopt unbiased algorithms, and continually monitor and adjust AI tools post-deployment to minimise biases. Properly designed AI systems, aligned with these ethical and procedural guidelines, can also move us closer to personalising medicine through factoring in patients’ protected characteristics. This requires incorporating considerations of bias and how these are tackled as part of the regulatory processes.AI tools must be trained on data that are representative of the population they serve, encapsulating characteristics such as age, ethnicity, gender, sexual orientation, and socioeconomic background. Nonetheless, current data collection methods have flaws that need re-evaluation and improvement. In the UK, the inpatient Hospital Episode Statistics (HES) system only contains 16 ethnic categories and is usually completed by third-person observation. Some other data are self-reported and the willingness of different demographic groups to participate can significantly limit the scope of inclusivity.8 In some countries, the challenges may be further compounded by cultural taboos surrounding discussions on ethnicity and race.Initiatives like STANDING Together, which aims to develop recommendations for dataset composition and reporting, can help in promoting data diversity.9 There is therefore a need for a harmonised quality standard—a digital fingerprint—that enables evaluators of projects and deployments to better understand the nature of the data used to train AI tools, which in many cases are proprietary and not accessible. Such digital fingerprints can be reliably computed using cryptographic methods even for proprietary given datasets and publicly reported. Furthermore, establishing partnerships with community organisations is another promising strategy. Through a two-way dialogue, these collaborations can enable developers to tailor AI tools to meet distinct health needs and preferences of different demographics during the stages of problem selection and outcome definition. Approaches like participatory design or “co-design” can expand acceptance and utilisation of AI tools once deployed.4Another strategy is to robustly evaluate how algorithms perform in various populations, through sensitivity checks, data stratification, and sub-population weighting.4 Sensitivity checks involve assessing algorithmic performance when certain variables or data subsets are altered, which can determine how different patient characteristics or clinical conditions can affect algorithmic predictions. On the other hand, data stratification entails dividing data into distinct sub-groups based on relevant criteria, such as religious affiliations, geographic location, socio-economic levels, or health status. This allows for a more nuanced understanding of the data and can mitigate potential biases that adversely affect diagnostic accuracy or treatment recommendations. Sub-population weighting can be employed to give higher importance to under-represented or more vulnerable groups. Beyond these direct algorithmic solutions, the evaluation itself should be systematised.A promising option is the establishment of digital healthcare testbeds, where developers can take their algorithms and have them evaluated in a comparable and systematic manner. Digital healthcare testbeds should be designed to offer rich and diverse datasets in secure data environments, so that the developer cannot take the data out, but instead can put their AI models in. Then automated assessment protocols can be run following a common set of criteria and procedures producing an independent evaluation of an AI tool’s capability and issues. By attuning to specific needs and health inequalities faced by different populations, these approaches ensure that AI tools are fostering fairer and more equitable healthcare outcomes.To tackle these challenges, developing a robust regulatory framework is pivotal to ensure AI tools adhere to rigorous equity standards. A pragmatic approach could involve establishing a Health Equity Advisory and Algorithmic Stewardship Committee. This initiative could be spearheaded by national health authorities, such as the Department of Health and Social Care (DHSC) in England, in collaboration with Integrated Care Systems (ICS). This committee, integral to Patient and Public Involvement and Engagement (PPIE), would set standards and oversee AI technology in healthcare, ensuring compliance with ethical and equity guidelines to safeguard patients’ interests. These standards will encompass strict assessments on how AI bias is identified and mitigated, along with stipulating the standards required for training data used in developing commercial AI technologies. Currently, the onus of implementing methods to reduce bias largely rests on the willingness of developers—a practice that is not always diligently pursued. The aim is to foster a more conscientious approach to managing bias among developers and promote transparency in AI tools' decision-making and operational mechanics across diverse demographic groups.The effectiveness of AI systems hinges on the quality and calibre of the data they are built on. If newer AI tools can demonstrate lesser bias than human decision-makers, they represent a significant leap towards equity. However, to leverage on the revolutionary potential of AI, we must prioritise rigorous data assessment, active community engagement, and robust regulatory oversight. Promoting equity in AI tools will not only improve healthcare, but more importantly reduce health inequalities and improve health outcomes for all.FootnotesCompeting interests: none declared.Acknowledgments: Imperial College London is grateful for support from the NIHR Applied Research Collaboration North west London, NIHR North west London Patient Safety Research Collaboration, and the NIHR Imperial Biomedical Research Centre. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.Funding Information: A.A.F. acknowledges the support of his UKRI Turing AI Fellowship (EP/V025449/1).Provenance and peer review: not commissioned, not peer reviewed.References↵Kumar Y, Koul A, Singla R, et al. Artificial intelligence in disease diagnosis: a systematic literature review, synthesizing framework and future research agenda. J Ambient Intell Humaniz Comput2022;•••:1-28.pmid:35039756↵Smith C, Barclay S, Department of Health and Social Care. £21 million to roll out artificial intelligence across the NHS. 2023.↵Celi LA, Cellini J, Charpignon M-L, et al., for MIT Critical Data. Sources of bias in artificial intelligence that perpetuate healthcare disparities-A global review. PLOS Digit Health2022;1:e0000022. doi:10.1371/journal.pdig.0000022 pmid:36812532OpenUrlCrossRefPubMed↵O’Brien N, Van Dael J, Clarke J, et al. Addressing racial and ethnic inequities in data-driven health technologies. 2022.↵Tat E, Bhatt DL, Rabbat MG. Addressing bias: artificial intelligence in cardiovascular medicine. Lancet Digit Health2020;2:e635-6. doi:10.1016/S2589-7500(20)30249-1 pmid:33328028OpenUrlCrossRefPubMed↵Guidance WHO. Ethics and governance of artificial intelligence for health.World Health Organization, 2021.↵Chen IY, Pierson E, Rose S, Joshi S, Ferryman K, Ghassemi M. Ethical machine learning in healthcare. Annu Rev Biomed Data Sci2021;4:123-44. doi:10.1146/annurev-biodatasci-092820-114757 pmid:34396058OpenUrlCrossRefPubMed↵Mathur R, Grundy E, Smeeth L. Availability and use of UK based ethnicity data for health research. 2013.↵Ganapathi S, Palmer J, Alderman JE, et al. Tackling bias in AI health datasets through the STANDING Together initiative. Nat Med2022;28:2232-3. doi:10.1038/s41591-022-01987-w pmid:36163296OpenUrlCrossRefPubMed Via Emmanuel Capitaine
Digital therapeutics (DTx) are a somewhat novel class of US Food and Drug Administration-regulated
Lionel Reichardt / le Pharmageek's insight:
Les thérapies numériques (DTx) sont une classe de logiciels réglementés par la FDA qui aident les patients à prévenir, gérer ou traiter des maladies. Dans cette étude, les chercheurs ont utilisé le traitement automatique du langage naturel pour caractériser les essais cliniques enregistrés sur les DTx et fournir des informations sur le paysage du développement clinique de ces nouvelles thérapies. Ils ont identifié 449 essais cliniques sur les DTx, initiés ou prévus entre 2010 et 2030, à partir de ClinicalTrials.gov, et ont analysé les données disponibles, y compris les durées d'essais, les lieux, les catégories MeSH, les inscriptions et les types de sponsors. Les critères d'éligibilité des essais ont été analysés à l'aide du modèle de sujet BERTopic, montrant que les essais sur les DTx excluent fréquemment les patients en fonction de l'âge, des comorbidités, de la grossesse, des barrières linguistiques et des déterminants numériques de la santé. Les résultats mettent en évidence les défis de la conception d'essais cliniques inclusifs sur les DTx et présentent des opportunités pour les cliniciens et les chercheurs. Une tableau de bord interactif est également fourni pour permettre aux lecteurs de mener leurs propres analyses.

Enterprise software companies are focused firmly on healthcare. If you want proof, look at how Oracle and Microsoft both backed up trucks loaded with money to buy health tech companies this year.

Lire l'article complet sur : www.mypharma-editions.com Via Rémy TESTON

Lyonbiopôle, le pôle de compétitivité santé de la région Auvergne-Rhône-Alpes, annonce le lancement de la seconde promotion de son Programme d'Accélération Santé. Fort du succès de la première édition menée sur 2022 et 2023, ce nouveau programme va proposer une offre d’accompagnement enrichie pour... Via Emmanuel Capitaine
|
From
www
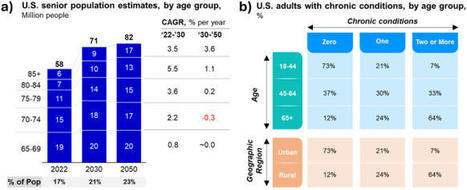
The US healthcare system is at a crossroads. With an aging population requiring more care and a strained system facing workforce shortages, capacity issues, and fragmentation, innovative solutions and policy reforms are needed. Via Emmanuel Capitaine

Le projet Neura, initié par le Dr Sami Barrit, médecin spécialiste en formation en neurochirurgie à l’ULB, représente une avancée notable dans le domaine de l'intelligence artificielle générative, appliquée spécifiquement aux sciences biomédicales. Une étude pilote en neurologie, où Neura a été confronté à des scénarios cliniques complexes, a démontré sa performance diagnostique par rapport à une cohorte de neurologues, avec des scores normalisés impressionnants de 86,17 % dans l'ensemble. Via Philippe Marchal

From
nyasowi
In the ever-evolving landscape of healthcare, the convergence of digital health and patient centricity is reshaping the way we approach medical services.Let’s delve into these two critical concepts, explore their significance, and understand how they intersect to enhance patient outcome... Via Emmanuel Capitaine
Lionel Reichardt / le Pharmageek's insight:
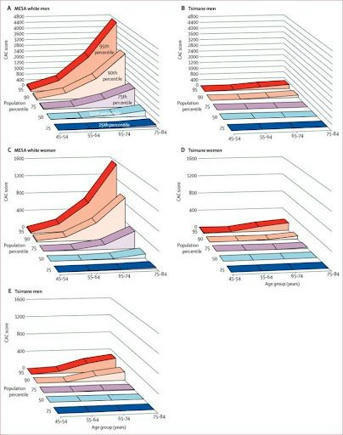
Le rôle de la mesure de la vitesse d'onde de pouls (VOP) dans l'évaluation de la santé cardiovasculaire est de plus en plus reconnu. La VOP mesure la vitesse à laquelle les ondes de pression se déplacent dans les artères, un indicateur précieux de la rigidité artérielle et un prédicteur significatif des risques de maladies cardiovasculaires. Une étude sur la population Tsimané montre une rigidité artérielle beaucoup plus faible, indiquant un système cardiovasculaire plus sain et plus jeune. L'utilisation de technologies comme le pOpmètre® d'Axelife permet d'identifier les patients les plus à risque et de détecter les premiers signes d'artériosclérose, afin d'améliorer leur santé cardiovasculaire.

La French Tech Grand Paris et le Digital Medical Hub via AP-HP révèlent en exclusivité les lauréats de la deuxième édition du programme e-santé Health Innovation Intensive Training (HIIT).Les startups sélectionnées bénéficieront d’un accompagnement gratuit et dédié lors du bootcamp HIIT*, réparti... Via Emmanuel Capitaine
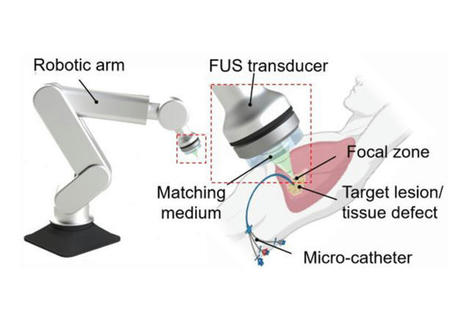
Des chercheurs de l'Université Duke et de la Harvard Medical School ont mis au point une méthode d'impression 3D à l'intérieur du corps humain, utilisant des ultrasons et une encre biocompatible. Via Philippe Marchal
From
www
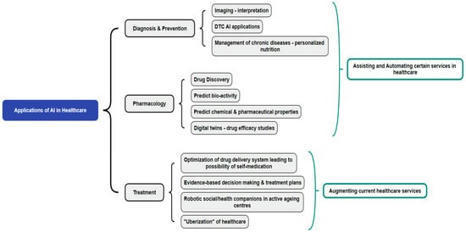
The healthcare sector is faced with challenges due to a shrinking healthcare workforce and a rise in chronic diseases that are worsening with demographic and epidemiological shifts. Digital health interventions that include artificial intelligence (AI) are being identified as some of the potential... Via Emmanuel Capitaine

Building AI tools into existing models is futile. It is time to go back to the drawing board, argues Orion Health's Brad Porter. Via Emmanuel Capitaine

En ayant recours à la bio-impression 3D, des chercheurs ont créé un dispositif pour mieux comprendre le comportement du coeur Via AXELIFE
Spécialisé dans le déploiement de logiciels de vigilances sanitaires, la société eVeDrug intègre l'IA pour optimiser ses solutions. Via Rémy TESTON

La marque française spécialisée dans les objets de santé connectés a deux grosses nouveautés produits : BeamO et U-Scan. En parallèle, son expansion l'entraîne à se rapprocher des gouvernements et des assureurs. Mais des limites persistent. Via Rémy TESTON

Lire l'article complet sur : www.healthcareittoday.com Via Emmanuel Capitaine
|